How to Naturally Heal Sciatica: 9 Root-Cause Interventions
Table of Contents
You have been stretching for three weeks and the pain is worse.
You did what the internet told you. You pulled your knee across your chest. You lay on your back and hugged your leg. You held the pigeon pose until your hip screamed. And somewhere around day ten, you noticed that the ache which used to stop at your buttock was now travelling past your knee.
This is not because you lack discipline. It is because you were handed a generic protocol for a condition that is not generic.
Here is the thing almost nobody will tell you when you search for how to heal sciatica naturally: sciatica is not a diagnosis. It is a symptom — a description of pain travelling along the path of a nerve. Underneath that symptom sit at least four distinct mechanisms, and they respond to opposite interventions. The movement that quietens one type of sciatica will inflame another. Which means that following the wrong protocol does not simply fail to help you. It actively makes you worse.
Your body is not malfunctioning. It is protecting a structure it believes is under threat, and it will keep sounding the alarm until that belief changes. The work is to find out what it is protecting, and then to give it a reason to stand down.
That is what this article is for.
Why Most Sciatica Advice Fails (And Why Stretching Might Be Making It Worse)

Open any of the top-ranking articles on natural sciatica relief and you will find the same list. Ice, then heat. The piriformis stretch. The knee-to-chest stretch. Some turmeric. Perhaps, if you are unlucky, celery juice or garlic milk.
The problem is not that these suggestions are exotic. The problem is that they are offered to everyone, unconditionally, as though every person with leg pain has the same thing wrong with them.
They do not. Broadly, sciatic symptoms arise through four different mechanisms:
Disc-related nerve root irritation. The most common cause of true sciatica. Material from a lumbar disc bulges or herniates and irritates the nerve root where it exits the spine. This kind of sciatica typically hates forward bending. Sitting is agony. Getting out of the car is worse. The pain often eases when you stand up and walk.
Deep gluteal or piriformis entrapment. The nerve is compressed further downstream, in the buttock, by muscle rather than by disc. This is far less common than the internet suggests. It typically produces deep buttock pain that worsens with prolonged sitting on a hard surface and with direct pressure on the glute.
Spinal stenosis. Usually a feature of an older spine. The canal through which the nerves travel narrows. This kind of sciatica is the mirror image of disc-related sciatica: standing and walking make it worse, and bending forward — leaning on a shopping trolley, sitting down — brings relief.
Sensitised or persistent sciatica. The imaging is clean, or the disc bulge that was there has resolved, and yet the pain continues. The tissue has healed. The alarm has not switched off.
Now look at the piriformis stretch — the single most recommended sciatica remedy on the internet.
To perform it, you lie on your back and pull your knee across your body toward the opposite shoulder. This does two things simultaneously: it flexes your lumbar spine, and it puts the sciatic nerve under tension.
If your sciatica is disc-related — statistically the most likely scenario — you have just done the two things most likely to provoke it. You have loaded the disc in the direction it least tolerates, and you have pulled on a nerve that is already irritated.
This is why so many people report that stretching made their sciatica worse. It is not a mystery. It is mechanics.
The first step in learning how to heal sciatica naturally is not to find a better stretch. It is to find out which kind of sciatica you actually have.
Which Type of Sciatica Do You Have? A Self-Triage Table
Read the row that matches your experience. The final column tells you which of the nine interventions below are most likely to apply to you.
| Pattern | What it feels like | Worse with | Better with | Likely mechanism | Start with |
| Flexion-intolerant | Sharp, electric pain down the back or side of the leg, often past the knee. Numbness or pins and needles. | Sitting, driving, bending forward, coughing, sneezing, getting out of a chair | Standing, walking, lying flat, gentle backward bending | Disc-related nerve root irritation | Interventions 1, 2, 3, 5, 6, 7, 8 |
| Extension-intolerant | Heavy, crampy, achy legs. Often both sides. Symptoms build the longer you stay upright. | Standing, walking, especially for long periods | Sitting, bending forward, leaning on a trolley or counter | Spinal stenosis | Interventions 2, 5, 6, 7, 8 |
| Pressure-sensitive | Deep, focal ache in the buttock. Pain may travel down the leg but often stays above the knee. | Sitting on hard surfaces, direct pressure on the glute, prolonged driving | Standing up, walking, taking weight off the buttock | Deep gluteal / piriformis entrapment | Interventions 3, 4, 5, 7, 8 |
| Non-mechanical | Pain that no longer follows a clear pattern. Flares with stress, poor sleep, or for no reason at all. Imaging clean or unchanged. | Unpredictable. Often stress, fatigue, fear of movement | Also unpredictable. Often distraction, good sleep, gentle activity | Sensitised nervous system (nociplastic pain) | Interventions 2, 5, 8, 9 |
If you fit two rows, you may have more than one thing going on — which is common, and which is precisely why generic advice fails.
Before you go any further: the red flags
Stop reading and seek emergency medical care today if you have any of the following:
- Numbness in the saddle region — the inner thighs, buttocks, or genitals
- Any change in bladder or bowel control, including difficulty urinating or loss of sensation
- Progressive weakness in one or both legs — a foot that drags, a knee that gives way
- Sciatic pain down both legs simultaneously, appearing suddenly
These can indicate cauda equina syndrome, a genuine surgical emergency in which delay causes permanent damage. This is not a case for natural remedies, patience, or a wait-and-see approach. It is a case for a hospital.
Everything else in this article assumes you have ruled these out.
9 Root-Cause Interventions to Heal Sciatica Naturally
1. Find Your Directional Preference — The Test Almost Nobody Tells You to Do
This is the most valuable ten minutes you will spend on your sciatica, and it appears in virtually none of the natural-remedy articles you will find online.
Clinicians who work with spinal pain use a concept called centralisation. The principle is this: when you move your spine repeatedly in the direction your body prefers, pain retreats toward the spine and away from the leg. When you move it in the direction your body dislikes, pain travels further down the leg. A systematic review of the evidence found that around two-thirds of people with back pain show a directional preference, and that its presence is a strong positive prognostic sign — people who centralise tend to recover better. Roughly a third show no clear direction at all. That matters, and we will come back to what it means.
The location of the pain is the feedback signal. Pain moving up toward your back — even if it briefly gets more intense there — is a good sign. Pain moving down toward your foot is a warning.
How to test it.
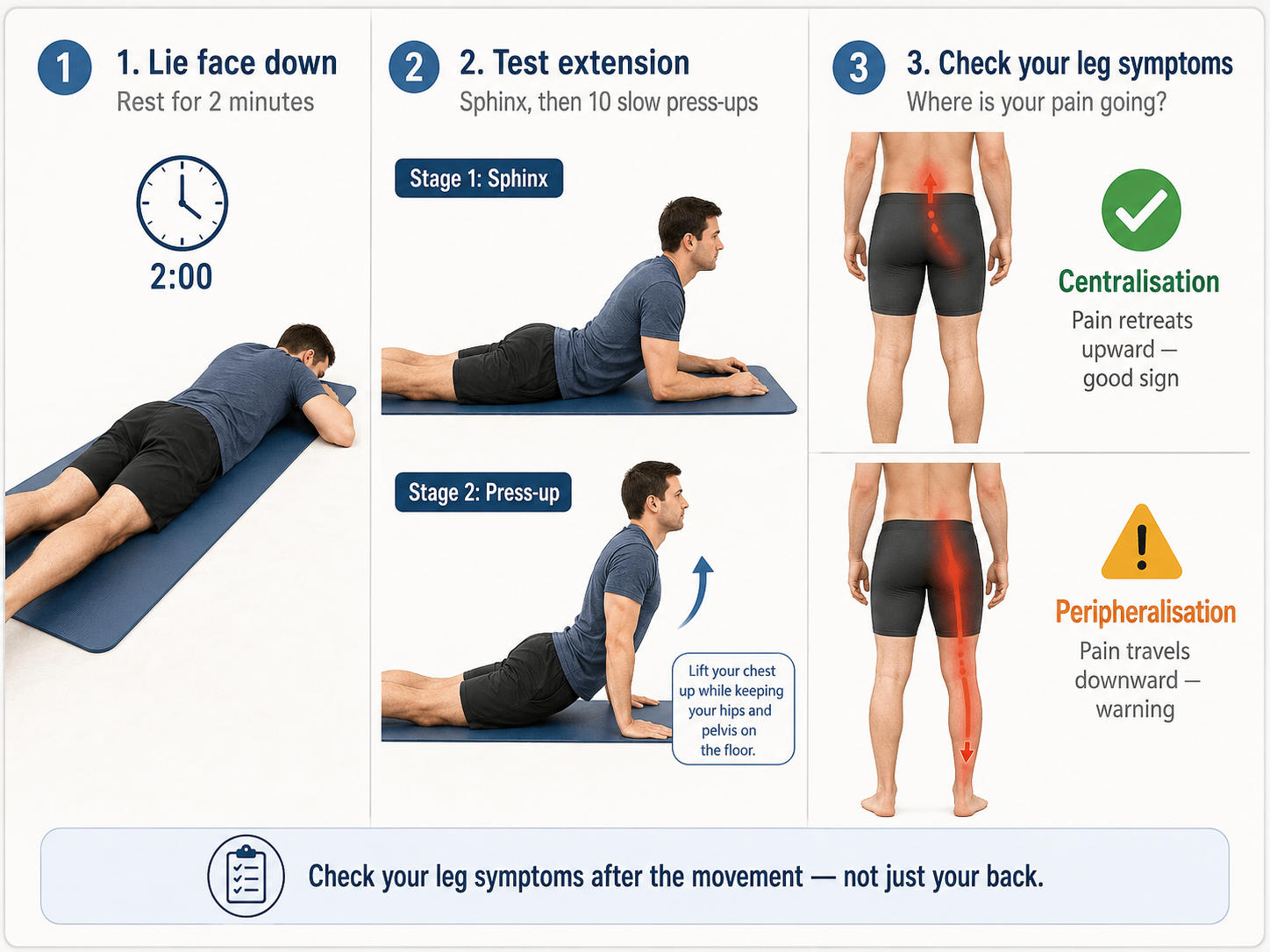
Lie face down on the floor for two minutes. Simply lie there. Then prop yourself on your forearms, like a sphinx, and rest there for another two minutes. Then, if that is tolerable, perform ten slow prone press-ups: hands under your shoulders, push your chest up while your hips stay heavy on the floor, and let your lower back sag. Come down between each one.
Now check your leg. Not your back — your leg.
- If the pain in your leg has receded upward, or the numbness has shrunk toward your buttock, you have an extension preference. Extension is your medicine. Repeat this several times a day, and treat forward bending with caution.
- If the pain has travelled further down your leg, stop. Extension is not your direction. Test the opposite: lie on your back, gently bring both knees to your chest, and repeat the check.
- If neither direction changes anything at all, your sciatica may be less mechanical than you think — go to intervention 9.
Do this test before you do anything else. It is the difference between a protocol that fits your body and a protocol you found in a listicle.
2. Stop Resting. Load Is the Medicine.
Every instinct you have is telling you to lie down and wait for this to pass.
Resist it.
Here the evidence deserves an honest hearing rather than a slogan. For acute low back pain, the Cochrane review is clear: people advised to rest in bed end up with slightly more pain and slightly less functional recovery than people advised to stay active. For sciatica specifically, the same review found little or no difference between the two approaches in the short term. So bed rest is not quite the villain some articles make of it. It simply has no upside — and it carries a real cost. Prolonged rest deconditions the muscles that support your spine, reduces the fluid exchange that keeps your discs nourished, and, most importantly, teaches your nervous system that movement is dangerous.
Your spinal discs have almost no blood supply. They are fed by diffusion: they absorb nutrients and expel waste through movement and load, like a sponge being squeezed and released. A still spine is a starving spine.
The protocol. Walk. Little and often, rather than one heroic effort. Five to ten minutes at a time, several times a day, is far more useful than a single forty-minute march that leaves you flattened. Increase the frequency before you increase the duration.
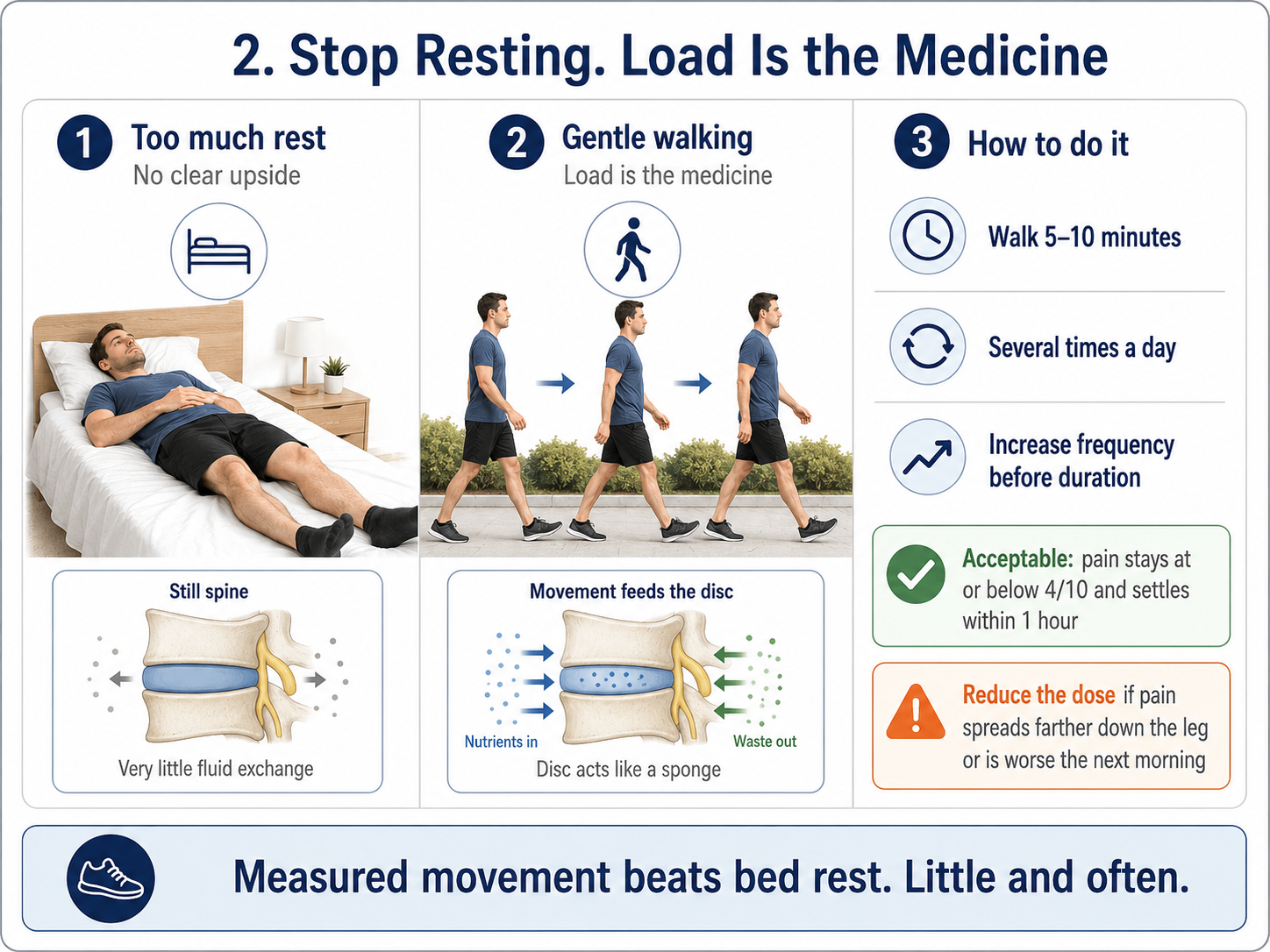
Some pain during walking is acceptable. A sensible rule: pain that stays at or below a 4 out of 10 during the walk, and settles within an hour afterward, is tolerable. Pain that spikes higher, spreads further down the leg, or is still elevated the next morning means you did too much. Reduce, do not stop.
This is not about pushing through. It is about giving your body the input it needs to remodel — a little more than yesterday, a little less than would provoke it.
3. Nerve Glides, Not Nerve Stretches
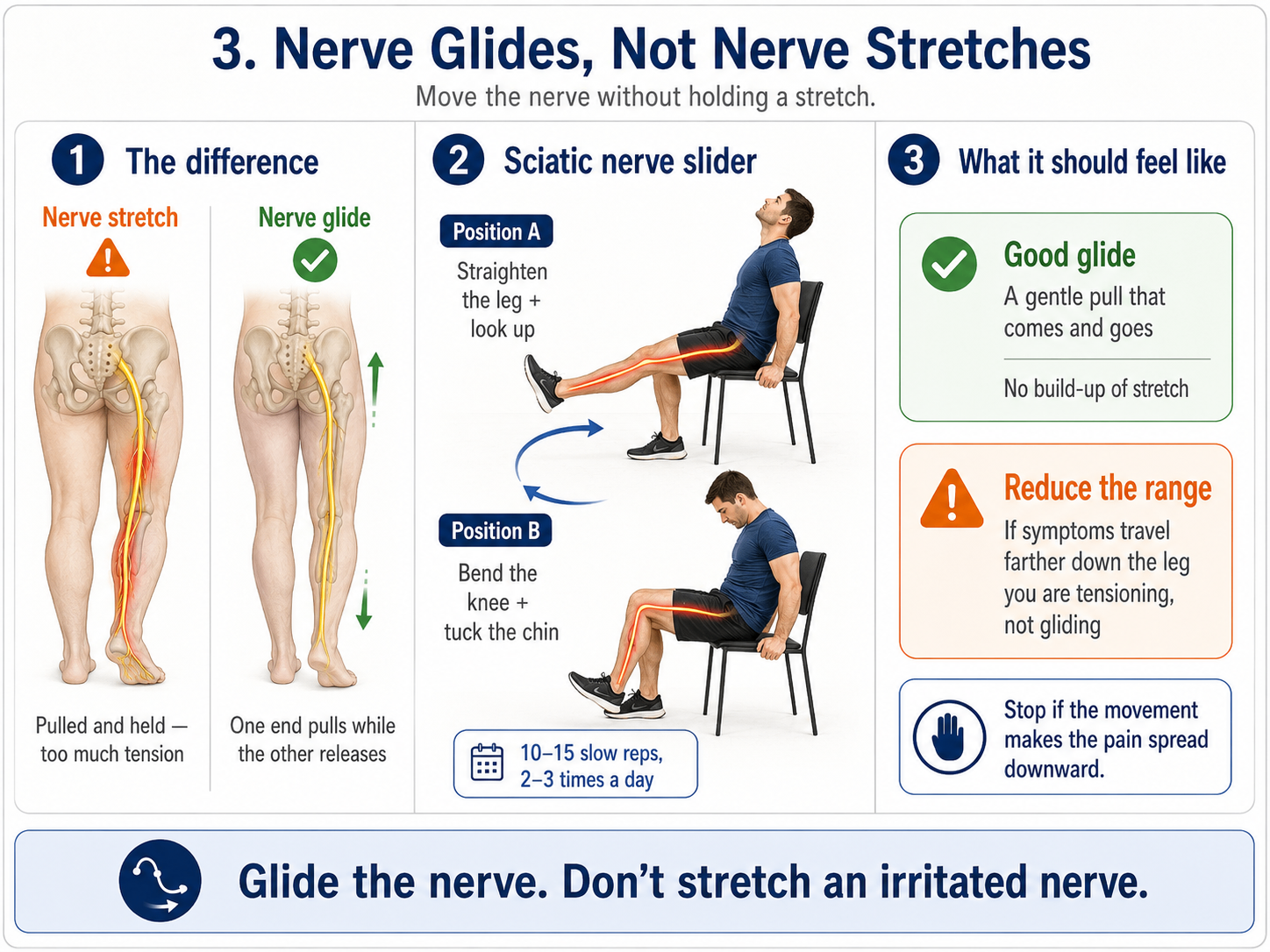
An irritated nerve does not want to be stretched. It wants to slide.
Nerves are not inert cables. They travel through tunnels of muscle and fascia, and they must glide freely as you move. When a nerve becomes irritated and inflamed, that gliding surface can become sticky and sensitive. The instinct is to stretch it — to pull it long and hold it there.
This is exactly wrong. Stretching an inflamed nerve is like pulling on a rope burn.
Instead, use a slider: a movement that pulls the nerve from one end while releasing it at the other, so it moves through its tunnel without ever coming under sustained tension.
Sciatic nerve slider. Sit upright in a chair with your feet on the floor. Now do two things at once: straighten your affected leg out in front of you while you tilt your head backward and look at the ceiling. Then reverse: bend the knee back down while you tuck your chin toward your chest. That is one repetition. It should feel like a gentle pull that comes and goes, never a stretch that builds.
Ten to fifteen slow repetitions, two or three times a day.
The rule that governs all of it: if symptoms travel further down your leg during or after the movement, stop. You are tensioning, not gliding. Reduce the range until only the sensation of movement remains.
4. Decompress the Deep Glute — If, and Only If, That Is Your Type
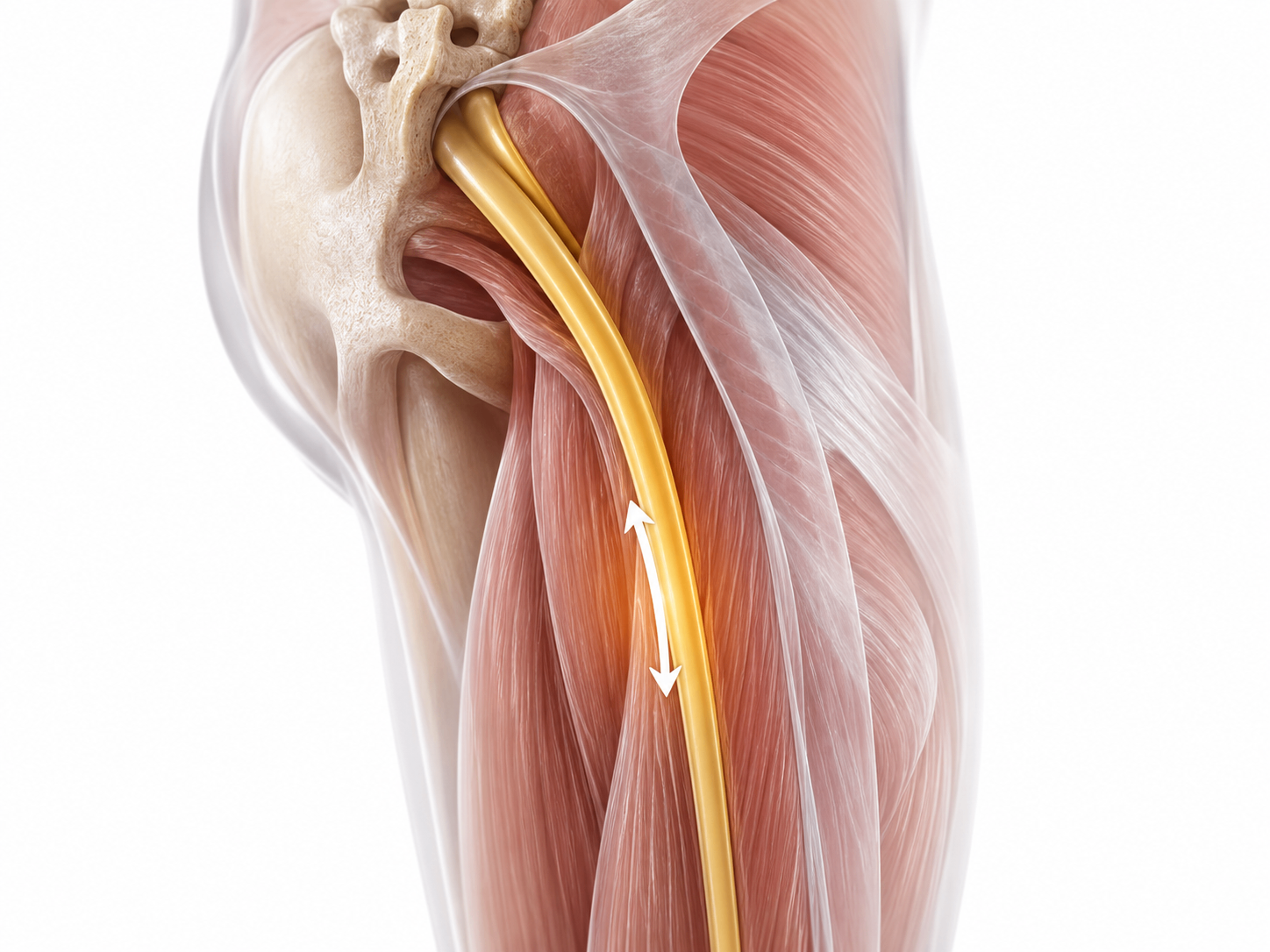
Now we can talk about the piriformis.
The piriformis is a small muscle deep in the buttock, and the sciatic nerve passes directly beneath it — or, in a minority of people, straight through it. When the muscle and surrounding tissue become tight or irritated, the nerve can be compressed there rather than at the spine.
If your triage row was pressure-sensitive — deep buttock ache, worse sitting on hard chairs, worse with direct pressure, generally not accompanied by the electric down-the-leg quality — then this is where your problem lives, and gentle release is genuinely appropriate.
Positional release, not aggressive stretching. Sit on a soft ball or a folded towel, positioned on the fleshy part of the buttock rather than on the bone. Apply gentle pressure. Breathe. Wait for the tissue to soften rather than forcing it. Sixty to ninety seconds, then move.
Follow this with hip mobility work rather than deep static stretching — controlled rotations, gentle figure-four positions held lightly, and hip movement through comfortable range.
If your triage row was flexion-intolerant — the disc pattern — skip this section. The piriformis is not your problem, and the classic stretch will likely aggravate the nerve root that is.
5. Rebuild Your Load Tolerance

There is a phrase in the wellness world that has been repeated so often it has stopped meaning anything: strengthen your core.
What it should mean is this: your spine is a structure that must tolerate load, and when its tolerance drops below the demands of your daily life, it protests. The goal is not a stronger stomach. The goal is a body that can carry, bend, lift, and sit without the nerve being provoked.
You raise load tolerance the way you raise any capacity: gradually, and with a pattern of stress and recovery.
Where to start, depending on your type:
- Flexion-intolerant (disc): Begin with movements that build stability without bending the spine. Dead bugs. Bird dogs. Side planks, scaled to your ability. Glute bridges. All of these teach the trunk to stay stable while the limbs move — which is precisely what your spine needs to relearn.
- Extension-intolerant (stenosis): Slight forward-flexed positions are often more tolerable. Cycling on a bike with a forward lean. Walking on an incline. Trunk work performed in a neutral-to-slightly-flexed spine.
- All types: Hip strength matters enormously and is chronically neglected. Strong glutes reduce the load your lumbar spine has to absorb with every step.
Progress slowly. Two sessions a week is enough to begin. This is the phase people rush, and rushing it is why sciatica recurs.
6. Fix the Sitting Load — Not the “Posture”

The ergonomic industry has sold you a myth: that there is a single correct posture, that your chair is the villain, and that if you simply sat properly your pain would resolve.
The research does not support a strong link between any specific sitting posture and back pain. What it does support is a link between prolonged static loading and symptoms.
The problem is not how you are sitting. It is how long you have been sitting in the same shape.
Sitting increases pressure on the lumbar discs, and it does so continuously. A disc under constant compression for ninety minutes has no opportunity to rehydrate. It is the duration that matters, not the angle of your pelvis.
The intervention is movement variability, not postural perfection.
- Change position every twenty to thirty minutes. Not dramatically — just shift.
- Stand up briefly every forty-five minutes. Ninety seconds is enough.
- Alternate between sitting positions rather than seeking one perfect one. A slightly reclined position, an upright position, a perched position — rotate through them.
- If you are flexion-intolerant, use a small lumbar support to reduce the flexed load on your discs. Not to force perfect posture — simply to reduce the amount of time your spine spends bent.
The best posture is the next one. Your body is designed for variability, not for stillness held with discipline.
7. Address the Inflammatory Terrain

An irritated nerve root sits in an inflammatory environment. The mechanical compression is only part of the story; the chemical irritation surrounding it is the other. This is why some people have significant disc herniations on imaging and no pain at all, and others have modest findings and severe symptoms.
You cannot mechanically decompress your way out of an inflammatory terrain. You can, however, change the terrain.
What has genuine support:
- Omega-3 fatty acids. Fatty fish, or a quality supplement. The evidence for reducing inflammatory pain is modest but real.
- Vitamin D. Deficiency is widespread and is associated with musculoskeletal pain. Worth testing rather than guessing.
- A genuinely anti-inflammatory diet. Not a marketing phrase — a real reduction in ultra-processed foods, refined seed oils, and added sugars, and a real increase in vegetables, fibre, and whole foods. Chronic low-grade inflammation is a systemic state, and it does not spare your spine.
- Magnesium. Reasonable for muscle tension and sleep quality. Do not expect it to resolve nerve compression.
- Turmeric / curcumin. Some evidence for inflammatory pain. Poorly absorbed on its own; requires an appropriate formulation.
What does not have support, despite appearing in most articles you will read:
Garlic milk. Celery juice. Aloe vera taken internally for nerve pain. Fenugreek seeds. These appear in high-ranking articles about sciatica because they are cheap to write about, not because there is any mechanism by which they would resolve a compressed nerve root. They will not hurt you. They will also not help you, and the time you spend on them is time you are not spending on the things that work.
Be sceptical of anyone who tells you that a kitchen ingredient will resolve a mechanical nerve compression. That is not root-cause thinking. That is a folk remedy with a wellness accent.
8. Sleep, Smoking, and the Metabolic Drivers Nobody Connects to Nerve Pain

This is where we get to the actual root causes — the upstream conditions that made your disc vulnerable in the first place, and that will determine whether this happens again in three years.
Smoking. If you smoke, this is the single highest-leverage change available to you. A meta-analysis of nearly 460,000 people found that current smokers carry a meaningfully elevated risk of lumbar radicular pain and clinically verified sciatica — while former smokers carry only a slightly elevated one. The risk, in other words, is largely reversible. The mechanism is straightforward: your discs are avascular and depend on nutrient diffusion through small vessels at their margins. Smoking constricts those vessels and impairs that diffusion. You are, in effect, starving the tissue that is trying to heal, and smokers recover from sciatica more slowly as a result.
Sleep. Insufficient sleep amplifies pain sensitivity, and this is not psychological. In controlled human studies, a single night of total sleep deprivation measurably increased pain sensitivity, impaired the body’s own descending pain-inhibition system, and made the spinal cord more excitable. A nervous system deprived of sleep turns the volume up on everything. Poor sleep also creates a vicious loop: pain disrupts sleep, and disrupted sleep amplifies pain. If your sleep has collapsed since your sciatica began, addressing it is not a nice-to-have. It is a direct intervention on your pain.
Metabolic health. Insulin resistance, elevated visceral adiposity, and chronic metabolic inflammation are all associated with worse disc health and greater back pain. The connection is rarely made in articles about sciatica, because sciatica is treated as a purely mechanical problem. It is not. A disc sitting in an inflamed, metabolically dysregulated body is a disc with less capacity to repair itself.
Load history. Sciatica rarely arrives without warning. It usually arrives after months or years of a body being asked to tolerate more than it had been prepared for — or, just as often, after months or years of a body being asked to tolerate almost nothing at all, and losing its capacity as a result.
These are the reasons this happened. The stretches address the symptom. This section addresses the cause.
9. Retrain a Nervous System That Has Stopped Turning the Alarm Off

Some sciatica does not resolve when the tissue does.
The disc bulge shrinks — and herniated discs do frequently resorb on their own, with reported spontaneous regression rates of roughly 96% for sequestrated discs, 70% for extrusions and 41% for protrusions. The inflammation settles. The imaging comes back unremarkable. And the pain continues, unchanged, sometimes for years.
This is not imagined pain, and it is not weakness. It is a real, physiological phenomenon: a nervous system that has become sensitised. Pain is not a direct readout of tissue damage — it is your brain’s output, its considered judgement about how much danger you are in. When that system has been running an alarm for long enough, it can learn to keep running it even after the threat has gone. The alarm has become the problem.
The signs: pain that no longer follows a clean mechanical pattern. Flares that track your stress levels rather than your activity. Pain that spreads beyond the original nerve distribution. Symptoms that worsen when you are frightened about them.
What actually helps here is different from everything above.
- Understanding the mechanism. This sounds soft. It is not. Pain neuroscience education — learning how pain is actually produced, that hurt does not equal harm, that a sensitised system can be desensitised — has been shown to reduce pain, disability and fear of movement in people with chronic pain. It works best when it accompanies the movement work rather than replacing it. Fear amplifies the alarm; understanding reduces it.
- Graded exposure. Slowly, deliberately reintroducing the movements you have been avoiding, in doses small enough that your nervous system does not sound the alarm. Bending. Lifting. Sitting. You are not testing your spine’s strength. You are teaching your nervous system that these things are safe again.
- Downregulating the whole system. Breathwork. Extended exhalation. Anything that shifts you out of a chronic protective state. A nervous system that is bracing all day is a nervous system that will keep the pain signal switched on.
If you have read this section and recognised yourself, this is likely the most important intervention in the article — and it is one you will not find on any of the pages selling you a stretch.
If you also have persistent lower back pain, this is the same mechanism expressing itself in a different place. The nervous system does not distinguish between the two. Treating them as separate problems is part of why neither resolves.
How Long Does It Take to Heal Sciatica Naturally?
Here is the honest answer, without the false comfort.
Most sciatica improves substantially without surgery — roughly nine in ten people recover without an operation, and most of them within a matter of weeks. That is genuinely good news, and it should temper the panic that a disc herniation on an MRI report tends to produce.
But “most” is not “all,” and “weeks” is not “days.”
A reasonable expectation looks like this. In the first two weeks, the goal is to stop making it worse — find your direction, keep moving, avoid the provocative positions. Between weeks two and six, the leg symptoms should begin to centralise, retreating upward toward the spine even as the back itself may feel more involved. That is progress, not deterioration. From six weeks to three months, you rebuild load tolerance and address the upstream drivers, and this is the phase that determines whether it comes back.
Numbness and pins and needles often resolve more slowly than pain. Nerves recover on their own timeline, and it is not always a fast one.
What natural approaches can do: resolve the mechanical provocation, reduce the inflammatory terrain, restore load tolerance, and desensitise an overprotective nervous system. That covers the substantial majority of cases.
What they cannot do: reverse a severe structural stenosis, resolve a large herniation causing progressive neurological loss, or substitute for surgery when surgery is genuinely indicated.
When Natural Sciatica Treatment Isn’t Enough
There is nothing holistic about ignoring a serious problem. Working with the body’s intelligence means listening to it — including when it is telling you that something is genuinely wrong.
Seek assessment if:
- Your symptoms are worsening rather than plateauing after four to six weeks of appropriate self-management
- You have progressive muscle weakness — a foot that catches on stairs, a leg that buckles
- Your pain is severe enough that you cannot sleep, work, or function, and is not improving
- You have any of the red flags listed earlier — those are an emergency, not a delay
A good clinician will not immediately reach for surgery. Most will confirm your mechanism, guide your loading, and work with the same principles described above. But they can assess what you cannot assess in yourself, and they can catch the small percentage of cases where a mechanical problem is genuinely progressing.
Knowing when to escalate is not a failure of the natural approach. It is part of it.
Your Body Is Not Broken
The most useful reframe available to you is this one: your sciatica is not a malfunction. It is a protective response, and a fairly intelligent one. Something in your spine or your buttock is irritated, and your nervous system is doing exactly what it evolved to do — making the movements that threaten that structure feel unbearable, so that you stop making them.
The problem is not that the alarm is sounding. The problem is that the alarm has been sounding for so long that it has forgotten how to stop, and that nobody has addressed the thing it was sounding about.
Find your direction. Keep moving. Glide the nerve rather than stretching it. Rebuild the tolerance you lost. Change the terrain your nerve is sitting in. Sleep. Stop smoking. And if the alarm has outlived the threat, teach your nervous system that it is safe to stand down.
That is how to heal sciatica naturally — not by silencing the signal, but by resolving what the signal is about.
Learn to Work With the Body, Not Against It
If reading this has changed how you think about pain — if the idea that symptoms are signals rather than malfunctions resonates with something you already suspected — you may be the kind of person who is drawn to helping others reach the same understanding.
Scholistico offers six internationally recognised certification programmes for people who want to build that knowledge properly and put it to work:
- Holistic Health Practitioner Certification — the systemic view of the body, and how to apply it
- Naturopathy Practitioner Certification — root-cause assessment and natural intervention
- Holistic Nutrition Consultant Certification — the inflammatory and metabolic terrain, in depth
- Movement Therapy Practitioner Certification — load, mobility, and the body’s capacity to adapt
- Sound Therapy Practitioner Certification — working with the nervous system through sound
- Art Therapy Practitioner Certification — the expressive and emotional dimensions of healing
Each is designed to be studied at your own pace, and each equips you to work with people the way you wish someone had worked with you.



Responses